
Page 16 - Venafi - 2021 Benefit Guide - CA
P. 16
medical, dental, and vision rates
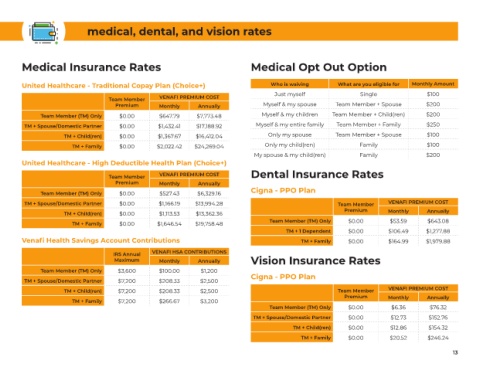
Medical Insurance Rates Medical Opt Out Option
United Healthcare - Traditional Copay Plan (Choice+) Who is waiving What are you eligible for Monthly Amount
Just myself Single $100
Team Member VENAFI PREMIUM COST
Premium Monthly Annually Myself & my spouse Team Member + Spouse $200
Team Member (TM) Only $0.00 $647.79 $7,773.48 Myself & my children Team Member + Child(ren) $200
TM + Spouse/Domestic Partner $0.00 $1,432.41 $17,188.92 Myself & my entire family Team Member + Family $250
TM + Child(ren) $0.00 $1,367.67 $16,412.04 Only my spouse Team Member + Spouse $100
TM + Family $0.00 $2,022.42 $24,269.04 Only my child(ren) Family $100
My spouse & my child(ren) Family $200
United Healthcare - High Deductible Health Plan (Choice+)
Team Member VENAFI PREMIUM COST Dental Insurance Rates
Premium Monthly Annually
Team Member (TM) Only $0.00 $527.43 $6,329.16 Cigna - PPO Plan
TM + Spouse/Domestic Partner $0.00 $1,166.19 $13,994.28 Team Member VENAFI PREMIUM COST
Premium Monthly Annually
TM + Child(ren) $0.00 $1,113.53 $13,362.36
TM + Family $0.00 $1,646.54 $19,758.48 Team Member (TM) Only $0.00 $53.59 $643.08
TM + 1 Dependent $0.00 $106.49 $1,277.88
Venafi Health Savings Account Contributions TM + Family $0.00 $164.99 $1,979.88
IRS Annual VENAFI HSA CONTRIBUTIONS
Maximum Monthly Annually Vision Insurance Rates
Team Member (TM) Only $3,600 $100.00 $1,200
TM + Spouse/Domestic Partner $7,200 $208.33 $2,500 Cigna - PPO Plan
TM + Child(ren) $7,200 $208.33 $2,500 Team Member VENAFI PREMIUM COST
Premium Monthly Annually
TM + Family $7,200 $266.67 $3,200
Team Member (TM) Only $0.00 $6.36 $76.32
TM + Spouse/Domestic Partner $0.00 $12.73 $152.76
TM + Child(ren) $0.00 $12.86 $154.32
TM + Family $0.00 $20.52 $246.24
13 13